The short version
A fishbone diagram (also called an Ishikawa or cause-and-effect diagram) organizes the possible causes of a problem into categories branching off a spine, with the problem at the head. In healthcare it does one essential job: it pushes a team past the reflex to blame a person and toward the system that let an error happen. This guide walks how to build one for a care-delivery problem — choosing categories that actually fit clinical work, brainstorming causes at the bedside with the people who do the work, going deep with the 5 Whys, and then verifying the vital few before you act. You'll finish able to facilitate your first fishbone session on a real problem this week — without it turning into a blame exercise or a wall of sticky notes nobody uses.
Why a fishbone is different in healthcare
Most fishbone examples come from a factory — the classic "6Ms" (Man, Machine, Method, Material, Measurement, Mother Nature). Care delivery breaks those assumptions, and that's why a copy-pasted manufacturing fishbone so often stalls in a hospital:
- The reflex is to blame the person, and that ends the investigation. When a medication error reaches a patient, the instinct is "who did this?" A fishbone's entire value is forcing the harder, more useful question: what about the system made this error easy to make and hard to catch? The frontline clinician is almost never the cause — they're the last layer of a system that failed upstream.
- The "6Ms" don't fit a ward. "Machine" and "Mother Nature" map poorly to clinical work. Care problems sort better into categories like People, Process, Equipment, Environment, Materials, and Communication — and getting the categories right is half the battle.
- A fishbone brainstorms; it doesn't conclude. It's a structure for surfacing possible causes comprehensively, so the team doesn't jump to the first plausible one. It pairs with the 5 Whys (to go deep) and root-cause analysis (to verify) — on its own it's a map of suspects, not a verdict.
- It only works in a safe room. Frontline staff won't name the real causes — the confusing label, the missing barcode scanner, the interruption-prone med room — if they fear the diagram will be used against them. Psychological safety isn't a nicety here; without it the bones fill with polite half-truths.
So the goal isn't a tidy diagram. Borrowing the Toyota lens: efficiency is the consequence, not the goal — and so is safety. You're after the genuine, changeable system causes, because fixing those is what actually protects the next patient.
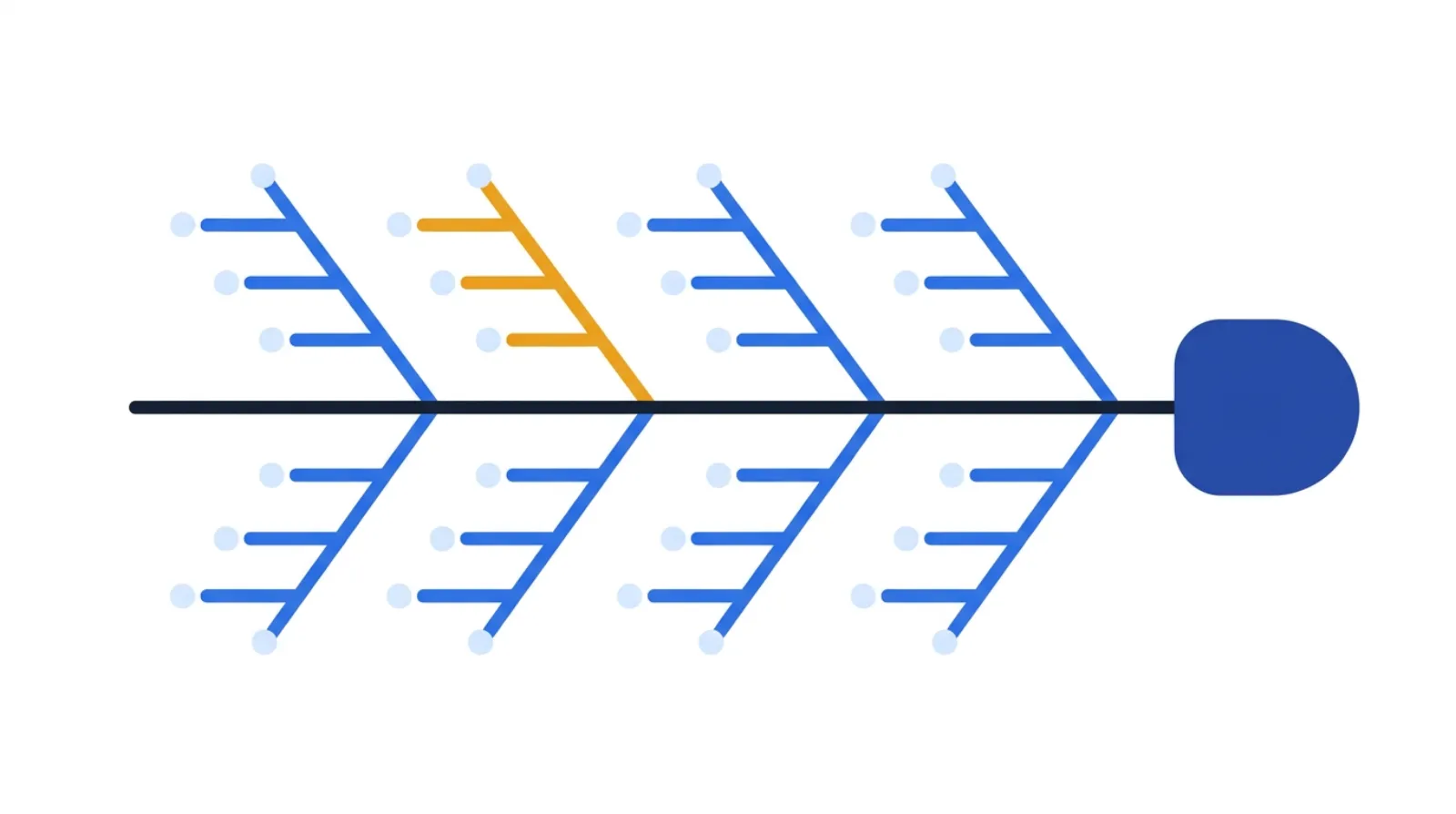 Six bones force a complete search; the highlighted one is the vital few the team will verify and act on.
Six bones force a complete search; the highlighted one is the vital few the team will verify and act on.
The one-line test for a healthcare fishbone: does every cause point at a system you can change, not a person you can blame? If a bone reads "nurse was careless," you haven't found a cause — you've stopped looking.
How to build the fishbone, step by step
A fishbone is a sequence, and skipping a step is where it goes wrong. Here's the order that holds up in a real review.
1Write the problem at the head — a sharp, measurable effect
The "head" of the fish is the problem statement, and a vague one dooms the whole diagram.
- State the effect, not a cause or a solution: "Wrong-dose insulin reached patients on Unit 4 three times last month," not "nurses need more training."
- Make it specific and, where you can, measurable — what, where, how often. A fuzzy head ("medication safety") produces a fuzzy, useless diagram.
2Choose categories that fit care delivery — the bones off the spine
The major "bones" are your cause categories. Pick ones that match clinical work rather than forcing the factory 6Ms.
- A reliable healthcare set: People (staffing, fatigue, competency), Process (the steps and handoffs), Equipment (pumps, scanners, IT systems), Environment (noise, interruptions, layout), Materials (drugs, labels, supplies), and Communication (orders, handoffs, documentation).
- Four to six bones is plenty. Too many categories fragment the thinking; too few crowd everything onto one bone.
3Brainstorm causes onto the bones — at the gemba, with the people who do the work
Now fill each bone with possible causes — and do it with the staff who actually do the task, ideally where the work happens.
- Go to the gemba — the med room, the ward, the OR — and look. Causes you'd never guess from a conference room ("the scanner won't reach the far bed") surface instantly on the floor.
- Brainstorm wide before you judge. Every plausible cause goes on a bone; no debating yet. Quantity first, filtering later.
- Keep asking "why might that happen here?" to push past generic causes toward the specifics of this unit.
4Go deeper on each promising bone — pair it with the 5 Whys
A single layer of causes is usually still surface-level. Take the candidates that look real and drill.
- Apply the 5 Whys to a promising cause: why did the label confuse the nurse? → two drugs have near-identical packaging → why are they stored together? → … Each "why" moves you from symptom toward a changeable system cause.
- Stop when you reach something you can actually act on — a storage rule, a label standard, a workflow — not a person's character.
5Find the vital few and verify — don't try to fix the whole diagram
A full fishbone has dozens of possible causes. You can't (and shouldn't) fix them all.
- Use data to find the vital few: which causes actually drive the problem? A Pareto view of incident data often shows a handful of causes behind most events.
- Verify before you act — a cause on the diagram is a hypothesis, not a fact. Check it against records, observation, or a small test. Then route the confirmed causes into corrective action, ideally mistake-proofed so the error becomes hard to make at all.
How to run your first fishbone session (step-by-step)
Don't try to boil the ocean. Pick one specific problem and run a focused 45–60 minute session.
- Frame the problem and invite the right people. Write a sharp effect statement; invite the frontline staff who do the work, not just managers. Set the tone explicitly: we're examining the system, not the people.
- Draw the spine and the bones. Problem at the head; label four to six care-fit categories as the major bones.
- Brainstorm onto the bones. Go wide, no judging. Capture every plausible cause under the best-fit category. Visiting the gemba first makes this far richer.
- Drill the promising causes. Apply the 5 Whys to the candidates that look real, pushing each toward a changeable system cause.
- Pick the vital few and verify. Use available data to prioritize; confirm the top causes before committing to fixes.
- Assign and follow up. Turn verified causes into corrective actions with owners and dates — and re-check whether the problem actually drops.
A focused session like this is the front half of an A3 — and it's the unit you repeat problem by problem.
A worked example: insulin dosing errors on a ward
To make the steps concrete, here's how a fishbone might play out for a real-feeling problem. The causes are an honest hypothetical — the moves are the ones you'd actually make.
Head (the effect): "Wrong-dose insulin reached patients on the unit three times last month."
The team draws six bones and brainstorms causes onto each, then drills the promising ones with the 5 Whys:
| Category (bone) | Example causes surfaced | Where the 5 Whys pointed |
|---|---|---|
| Communication | Verbal dose changes not documented promptly | Handoff lacked a standard for confirming insulin changes |
| Materials | Two insulin products with near-identical packaging | The two are stored side by side in the same bin |
| Equipment | Barcode scanner can't reach the far bed | Workflow lets staff skip the scan "just this once" |
| Process | Dose double-check done inconsistently under load | The check isn't built into the workflow, it's a habit |
| Environment | Med room interruptions during preparation | No quiet-zone or do-not-interrupt convention |
| People | Cross-covering staff unfamiliar with the unit's layout | Onboarding doesn't cover med-room specifics |
None of these is "the nurse was careless." Each points at a system the team can change — a storage rule, a label or look-alike-drug separation, a hard-stop on the scan, a built-in double-check, a quiet med room. The diagram's job is done not when it's full, but when the team can point to the vital few causes worth verifying and fixing first. Make the right action the easy one, and the error gets harder to make — which is what actually protects the next patient, no extra vigilance required.
Build your own on the same canvas the pros use — it opens on a worked patient-discharge example you can edit, or clear it and start from your own problem:
A simple fishbone health check
Before you trust a fishbone — or act on it — walk it against these five questions:
- Sharp head? Is the problem stated as a specific, measurable effect, not a vague theme or a pre-baked solution?
- Care-fit categories? Do the bones match clinical work (People, Process, Equipment, Environment, Materials, Communication) rather than the factory 6Ms?
- Built with the frontline, at the gemba? Did the people who do the work fill the bones, ideally where the work happens?
- Deep, not just wide? Were the promising causes drilled with the 5 Whys until they reach a changeable system cause?
- Verified vital few? Have you used data to prioritize and confirmed the top causes before committing to fixes?
You can build and share the diagram with the free fishbone tool — no whiteboard photos, no login.
Common healthcare fishbone mistakes
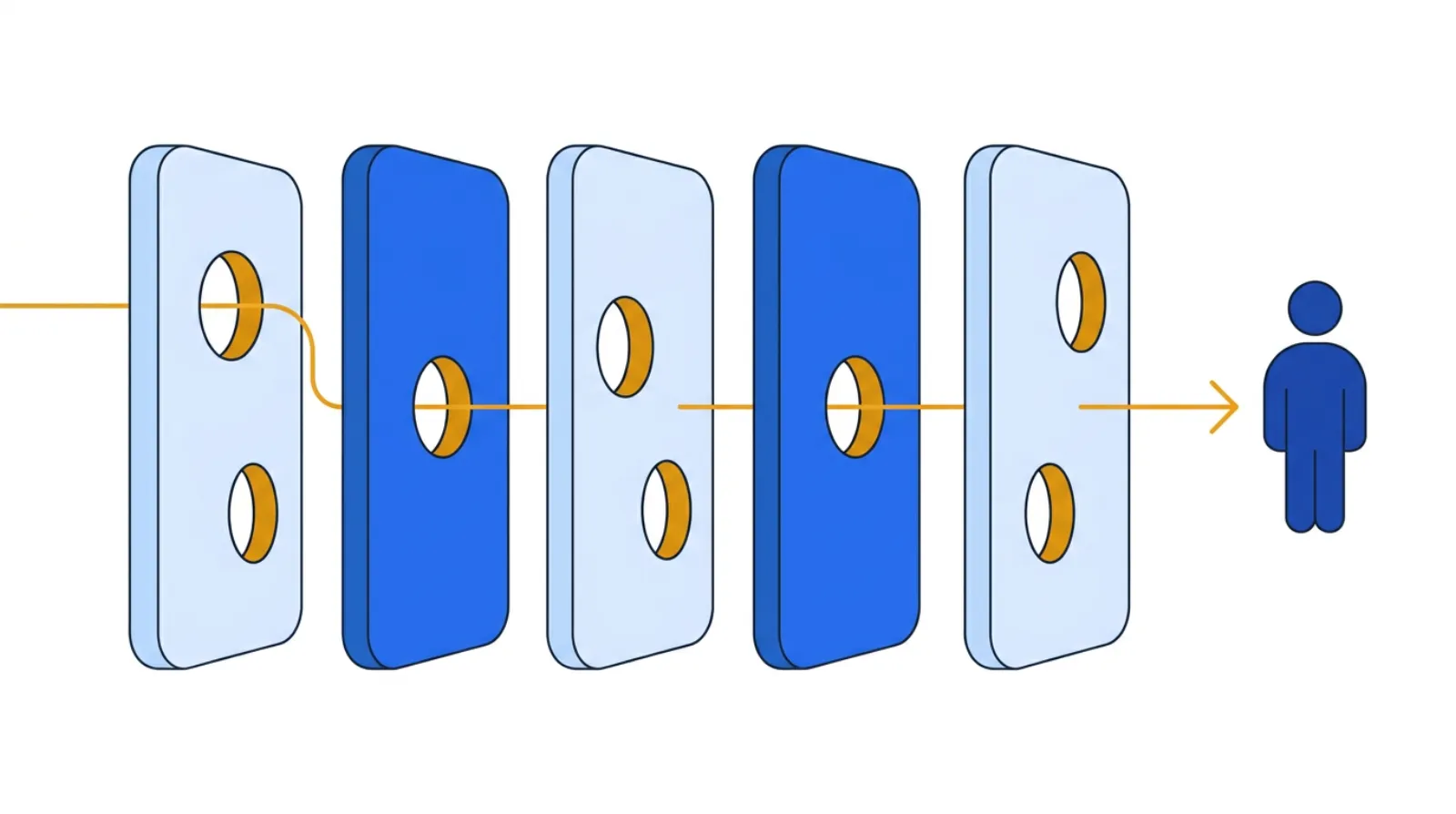 The error slips through aligned gaps in upstream defenses — the person at the sharp end is the last layer, not the cause.
The error slips through aligned gaps in upstream defenses — the person at the sharp end is the last layer, not the cause.
- Blame disguised as a cause. "Staff didn't follow policy" is where the analysis starts, not ends. Ask why the system made not-following easy.
- Stopping at the first layer. A bone that says "communication breakdown" isn't actionable. Drill it with the 5 Whys until you reach something you can change.
- Building it in a conference room. Causes brainstormed away from the work miss the obvious physical ones. Go look at the med room, the ward, the device.
- Filling the diagram and calling it done. A full fishbone is a list of suspects. Without prioritizing and verifying the vital few, it's wall art.
- No psychological safety. If staff fear the diagram will be used against them, the real causes never make it onto a bone. Set — and protect — a just-culture tone.
- One person drawing it alone. A fishbone is a team-thinking tool. Solo, it just reflects one person's assumptions.
Templates & tools
- Free fishbone tool — drop the problem at the head, build out the bones, and capture causes by category. No login required.
- Related: 5 Whys for drilling each bone, and root-cause analysis for verifying before you act.
FAQ
What is a fishbone diagram used for in healthcare? To organize the possible causes of a problem (a medication error, a fall, a delay) into categories so a team explores the whole system before jumping to conclusions — and so the analysis stays on system causes rather than individual blame.
What categories should a healthcare fishbone use? The factory "6Ms" fit poorly. A reliable care-delivery set is People, Process, Equipment, Environment, Materials, and Communication. Adapt to your problem — four to six well-chosen bones beats a rigid template.
What's the difference between a fishbone and the 5 Whys? A fishbone goes wide — it surfaces many possible causes across categories. The 5 Whys go deep — they drill one cause toward its root. They're complementary: use the fishbone to map suspects, then the 5 Whys to drill the promising ones.
Is a fishbone the same as root cause analysis? No. A fishbone is one tool used within root-cause analysis. It helps generate and organize candidate causes; RCA also requires drilling, prioritizing, and verifying the actual root cause before acting.
How do I keep a fishbone session from becoming a blame game? Set a just-culture tone explicitly, invite frontline staff as contributors, and apply the one-line test to every bone: does this point at a system we can change, not a person to blame? Reframe any "person" cause into the system question behind it.
Related concepts & guides
- Dictionary: Fishbone Diagram · Ishikawa Diagram · 5 Whys · Root-Cause Analysis · A3 Problem Solving · Pareto Chart
- Guides: How to Do 5S in Healthcare — the standardized, safer environment that prevents many of the causes a fishbone surfaces.
Sources
- Ishikawa, K., Guide to Quality Control — the origin of the cause-and-effect diagram.
- American Society for Quality, Fishbone (Ishikawa) Diagram
Related concepts
Founder of Kaizumi, an AI-powered Lean training platform. More about Matt →
Drafted with AI assistance and reviewed by Matt Savas for accuracy.