The short version
An A3 is a single sheet that walks one problem from a sharp problem statement, through the current state and root cause, to tested countermeasures and a follow-up plan. In healthcare the discipline matters more than the paper: the pull to skip straight to "let's add a checklist" is strongest exactly where a missed root cause can harm a patient. This guide shows how to run an A3 on a real clinical problem — a problem statement that survives scrutiny, a current state grasped at the bedside instead of the conference room, root-cause work that resists blaming the nurse, and countermeasures you prove on one unit before you spread them. You'll finish able to take one recurring problem and draft a credible A3 this week. For the method itself — watching an A3 get written, erased, and rebuilt — see the interactive A3 guide.
Why A3 problem solving is different in healthcare
Most A3 examples come from a factory: a defect rate, a changeover time, a line that stops. The method transfers, but the setting changes what's hard about it — and a copy-pasted manufacturing A3 stalls in a hospital for reasons that are specific to clinical work.
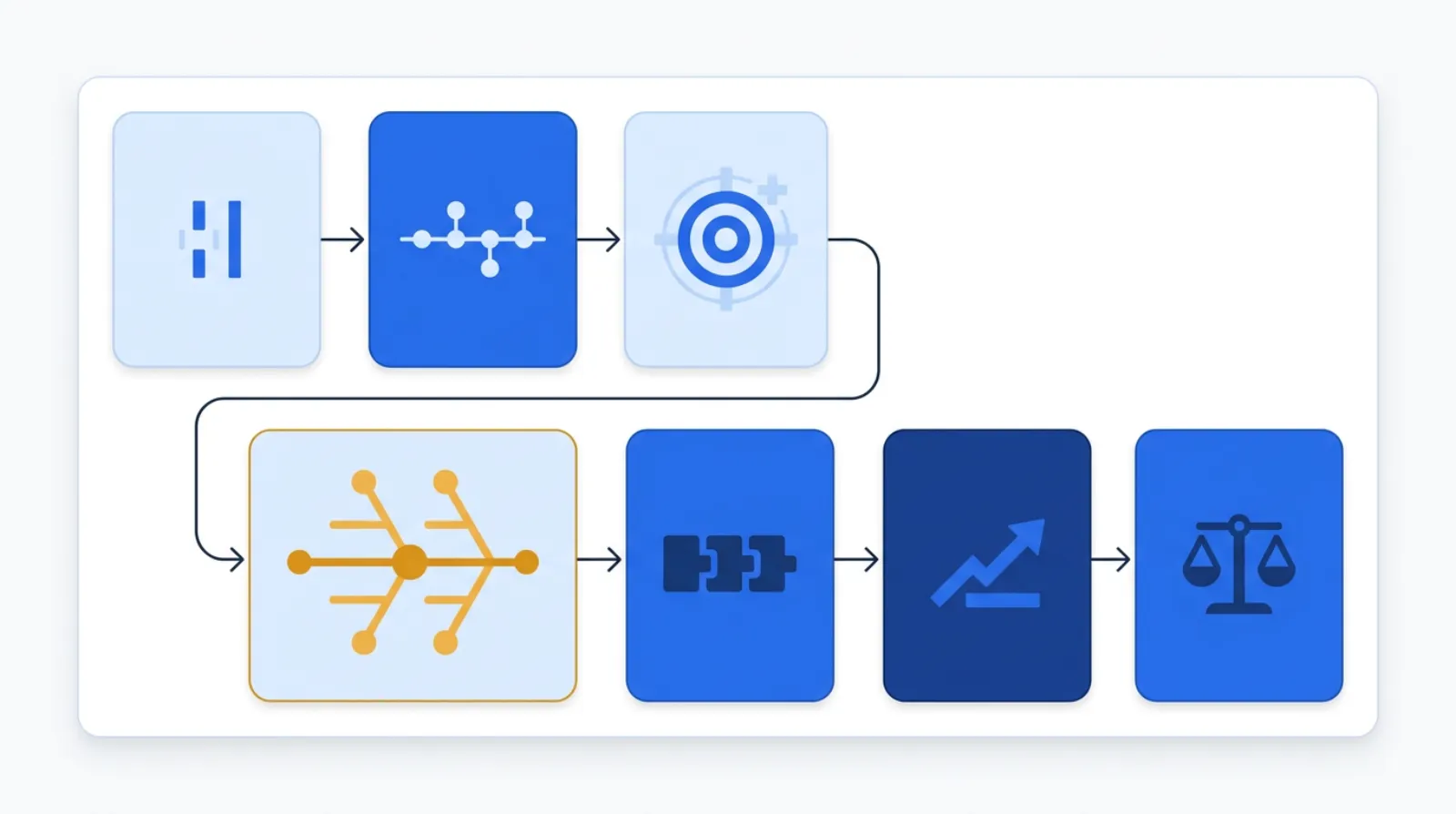 One sheet, seven linked boxes: the left half grasps the problem, the right half acts on it.
One sheet, seven linked boxes: the left half grasps the problem, the right half acts on it.
The one-line test for every A3 in a hospital: have you grasped the current state at the bedside, or are you solving the version of the problem you imagined in a meeting room? If you can't describe what actually happens on the unit, minute by minute, you're not ready to write countermeasures.
- The "defect" is a patient, so the pull to jump to a fix is overwhelming. When the problem is a missed medication or a fall, the instinct is to act now — add an alert, add a form, retrain the nurse. A3 forces a pause that feels uncomfortable in a clinical culture wired to intervene. That pause is the point: untested countermeasures pile alert fatigue and extra steps onto already-overloaded staff.
- Root cause hides behind the person at the sharp end. The nurse who hung the wrong bag, the resident who missed the page — they're the easiest thing to see and the worst place to stop. Healthcare A3 has to push past the individual to the system: the look-alike labels, the interrupt-driven workflow, the order set that defaults wrong. Blaming the person ends the investigation right where it should start.
- The current state is genuinely invisible. A factory problem leaves WIP stacked on the floor. A clinical problem — a delayed discharge, a lab result nobody saw — lives in the EHR (electronic health record) timestamps, handoffs, and waiting that no single person witnesses end to end. You have to reconstruct it deliberately.
- Standardizing is a clinical-governance act, not a memo. A countermeasure that changes how care is delivered touches protocols, scope of practice, and safety sign-off. "Make it standard" means working through the people who own the protocol — it can't be a poster taped to the med room wall.
So the goal isn't a tidy document. Borrowing the Toyota lens: efficiency is the consequence, not the goal. You're after safer, easier, more reliable care — and the A3 is the thinking tool that gets a team there together, with respect for the people doing the work.
The seven boxes of an A3, translated for healthcare
An A3 isn't a free-form report — it's a left-to-right story that mirrors PDCA (Plan-Do-Check-Act, the four-step improvement loop): the left half (Plan) grasps the problem, the right half (Do-Check-Act) tests and locks in the fix. Here's what goes in each box on a clinical problem.
1Problem statement — name the gap, not the solution
The single most common A3 failure is a problem statement that's actually a hidden solution ("we need a sepsis alert"). State the gap instead: what's happening versus what should be, in measurable terms, for a specific population. "On the medical-surgical unit, 18% of sepsis bundles miss the three-hour antibiotic window; the target is under 5%." (A sepsis bundle is the set of timed steps a patient is supposed to get — recognition, cultures, antibiotics, fluids — within a fixed window.) No cause, no fix — just the gap. If your statement names a countermeasure, you've ended the investigation before it started.
2Background — why this problem, why now
A sentence or two on why this matters and why it's worth the team's time: the patient-safety stakes, the regulatory or accreditation pressure, the link to the unit's bigger goals. Background earns the A3 its place against everything else competing for attention. Adults engage with a problem when they understand why it's worth solving — so make the "why now" honest and concrete.
3Current state — grasp it at the gemba, not in a meeting
This is where healthcare A3s live or die. Gemba is the Japanese term for "the actual place" — where the work really happens, which for you means the unit, not the conference room. Go see the actual work: walk the sepsis bundle from recognition to antibiotic, follow the EHR timestamps, watch a real case unfold. Draw what actually happens — the interruptions, the waiting, the rework — not the policy version. Quantify it: where do the minutes go, how often does each step fail. A current state grasped at the bedside almost always looks nothing like the flowchart in the policy binder.
4Goal — a measurable target with a date
Turn the gap into a target: the metric, the number, the deadline. "Cut bundle misses from 18% to under 5% on this unit within 90 days." Specific enough that anyone can tell whether you got there. A goal without a number is a wish, and a wish can't drive a kaizen — a small, structured improvement effort.
5Root cause — get past the nurse to the system
Now ask why the gap exists, and keep asking. Use the 5 Whys to drill a single chain, or a fishbone diagram to map causes across people, process, equipment, and environment. The discipline in healthcare is to route around the individual and into the system: not "the nurse didn't recognize sepsis" but "recognition depends on a vitals pattern no one is cued to, on a unit with a 1:6 ratio at night." That's root-cause analysis doing its real job — finding the condition that made the error likely, not the person who was standing there when it happened.
6Countermeasures — change the conditions, then test small
Countermeasures attack the root cause, not the symptom. Favor ones that change the conditions of work: mistake-proofing the order set so the wrong dose can't be selected, surfacing the vitals pattern automatically, removing an interruption rather than asking people to ignore it. Then test on one unit, one shift before you spread — a small experiment, not a hospital-wide rollout. Untested countermeasures are how you get alert fatigue.
7Follow-up — confirm it held, then standardize
Plan the check: when you'll measure, what tells you it worked, what you'll do if it didn't. If the countermeasure holds, lock it into standard work and the protocol — which in healthcare means working through the people who own clinical governance, not pinning a sign in the break room. If it didn't, the A3 isn't a failure; it's a learning, and you cycle again.
How to run your first clinical A3 (step-by-step)
Pick one recurring, bounded problem — not "patient safety," but "missed sepsis antibiotic windows on 4 West." One problem, one sheet, one owner.
- Choose the problem and the owner. A clear, recurring gap on a defined unit, with one person accountable for thinking it through (not necessarily fixing it alone).
- Write the gap, not the fix. Draft the problem statement as a measurable gap for a specific population. Read it back: if it names a solution, rewrite it.
- Go see the current state. Walk the process at the gemba with the people who do the work. Reconstruct the real timeline from the bedside and the EHR, and draw it — interruptions and rework included.
- Set a measurable goal. A number and a date that closes the gap you named.
- Find root cause with the team. Run 5 Whys or a fishbone with the frontline staff, and keep pushing past the individual to the conditions of the work.
- Design and test countermeasures small. Pick changes that alter the conditions, run them on one unit/shift, and measure. Then plan the follow-up: confirm it held and standardize through governance, or learn and cycle again.
A worked example: missed sepsis bundles on a med-surg unit
Here's how a first A3 tends to take shape. The numbers are an honest hypothetical — the shape of the reasoning is what you'll actually use.
Problem statement. On the med-surg unit, 18% of sepsis bundles miss the three-hour antibiotic window; the target is under 5%.
You go see the current state — walk three recent cases with the charge nurse and a staff nurse, and trace the EHR timestamps for each step:
| Step | What you observed | Where time/failure hides |
|---|---|---|
| Recognition | Vitals trend toward sepsis but no single cue flags it | Pattern spread across separate readings; night ratio 1:6 |
| Order entry | Provider paged, often mid-round | Page-to-order gap averages 40+ min |
| Pharmacy verify | Antibiotic verified after other queued orders | No priority flag on the order |
| Administration | Nurse retrieves, double-checks, hangs | Interrupted twice on a typical run |
Walk the 5 Whys on the biggest gap — recognition to order — and you don't land on "the nurse missed it." You land on: the deteriorating-vitals pattern isn't surfaced anywhere, so recognition depends on one busy person mentally connecting readings taken hours apart, on a unit running a heavy night ratio. That's a system condition, not a personal failing — and it's where the countermeasures belong.
So the targets are obvious, and none of them is "tell the nurses to be more vigilant." Surface the sepsis vitals pattern automatically so recognition doesn't depend on memory. Add a priority flag that pulls the antibiotic to the front of the pharmacy queue. Protect the administration step from interruption. Test all three on this one unit for two weeks, measure the window-miss rate, and only then decide what to standardize through clinical governance. Crucially, the gains come from changing the conditions of the work — not from asking exhausted people to try harder.
A simple A3 health check
You don't redraw a full A3 every week — but before a team presents one, walk it against six questions. Keep it to one page so it actually gets used:
- Gap, not fix: Does the problem statement name a measurable gap — or has a solution sneaked in?
- Gemba: Was the current state grasped at the bedside, or assembled from memory in a meeting?
- Past the person: Does root cause reach a system condition, or does it stop at "the nurse/resident didn't…"?
- Linkage: Do the countermeasures actually attack the root cause you found — or a different, easier one?
- Tested small: Were countermeasures proven on one unit/shift before any spread?
- Follow-up: Is there a date, a metric, and a plan for what happens if it didn't work?
If any answer is shaky, the A3 isn't ready to scale — and that's a far cheaper place to catch it than after a hospital-wide rollout.
Common healthcare A3 mistakes
- Solving in the problem statement. "We need a sepsis alert" isn't a problem — it's a fix in disguise. Name the gap and let the investigation choose the fix.
- Grasping the current state from a chair. The policy flowchart is the official story; the gemba is the real one. An A3 built on the binder version solves an imaginary problem.
- Stopping root cause at the person. Blaming the nurse or resident ends the inquiry exactly where the system causes begin. Push past the individual every time.
- Skipping the test. Rolling a countermeasure hospital-wide without proving it on one unit is how you manufacture alert fatigue and extra steps — new waste layered on the old.
- No follow-up. An A3 without a check date is a story with no ending. Confirm it held, standardize through governance, or learn and cycle again.
- Making it a solo report. An A3 written alone and presented for approval misses the point. It's a shared thinking tool — built with the frontline staff who own the work.
Templates & tools
- A3 problem solving — the full reference for the seven boxes and the thinking behind them.
- 5 Whys and the fishbone diagram — the two root-cause tools that fill the A3's center box; pair them on complex clinical problems.
- A free A3 worksheet and the rest of Kaizumi's lean tools live at kaizumi.com/tools — start with the root-cause tools above to build the heart of your sheet.
FAQ
What is A3 problem solving in healthcare? It's a structured, one-page method for working a clinical problem from a measurable gap, through current state and root cause, to tested countermeasures and follow-up. The single sheet mirrors the PDCA cycle and forces a team to understand a problem deeply before acting — which matters most in care settings where an untested fix can add risk and burden for staff and patients.
How do I write an A3 problem statement for a clinical problem? State the gap, not the solution: what's happening versus what should be, with a number, for a specific population — for example, "18% of sepsis bundles miss the three-hour antibiotic window on the med-surg unit; target under 5%." If your statement contains a fix ("add an alert"), rewrite it; the countermeasure is chosen later, after root cause.
What goes in each box of a healthcare A3 report? Seven linked boxes: problem statement (the gap), background (why now), current state (what actually happens at the bedside), goal (a measurable target with a date), root cause (the system condition behind the gap), countermeasures (changes that attack that cause, tested small), and follow-up (how you'll confirm it held and standardize).
Why not just add a checklist or an alert? Because a countermeasure that doesn't trace to root cause usually adds burden without removing the problem — and stacked alerts cause alert fatigue, which makes care less safe, not more. A3 makes you find the system condition first and test the fix on one unit before spreading it.
How is an A3 different from root cause analysis? Root-cause analysis is one step inside an A3 — the center box. The A3 wraps that analysis in the full arc: framing the gap, grasping the current state, setting a goal, designing and testing countermeasures, and following up. RCA finds the cause; the A3 turns it into a proven, standardized change.
Related concepts & guides
- Dictionary: A3 Problem Solving · PDCA · Root-Cause Analysis · 5 Whys · Fishbone Diagram · Gemba Walk · Standard Work · Poka-Yoke
- Guides: How to Use a Fishbone Diagram in Healthcare for the root-cause box, and How to Run a Value Stream Map in Insurance for grasping a current state across handoffs.
Sources
- Lean Enterprise Institute, Lean Lexicon: A3 Report
- Institute for Healthcare Improvement, Quality Improvement Essentials Toolkit
Related concepts
Founder of Kaizumi, an AI-powered Lean training platform. More about Matt →
Drafted with AI assistance and reviewed by Matt Savas for accuracy.